
Authored by Ian Miller via the Brownstone Institute,

“The Experts™” have repeatedly tried to deflect from the failure of their policies with misdirection.
The reason lockdowns didn’t work in the United States or the United Kingdom is because they weren’t strict enough, according to many in the expert community.
Of course, their excuses have been conveniently ignored as China’s repressive zero COVID lockdowns have continued, with horrific consequences.
Now that mass protests have broken out in the country that “The Experts™” revered for their COVID handling, there’s a massive effort to disregard their own previous advocacy.
This is perhaps best exemplified by Canadian Prime Minister Justin Trudeau, who clearly used authoritarian measures to suppress the protests in his own country, while now supporting Chinese demonstrations.
— Defiant L’s (@DefiantLs) November 30, 2022
The bewildering lack of awareness of their own hypocrisy seems to be a feature of COVID-obsessed politicians and public health authorities.
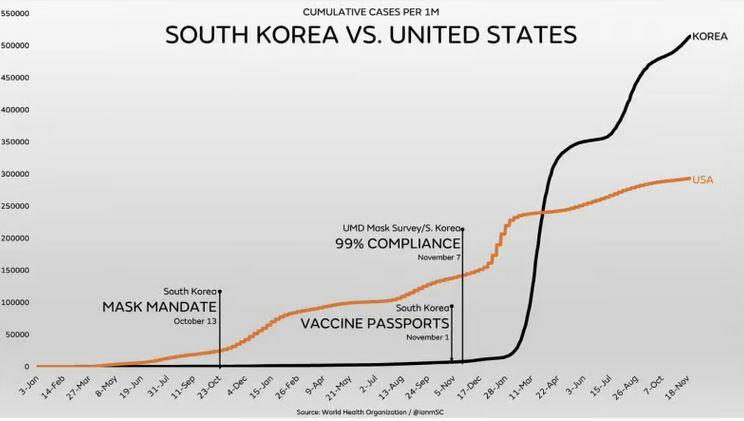
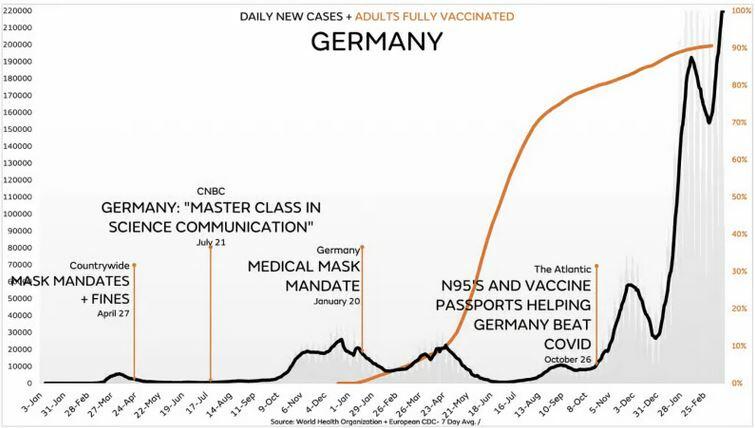
Another similar, oft-repeated assertion is that the failure of universal masking can be explained by the type of masks being used by the public.
Even though the CDC and Dr. Fauci explicitly claimed that wearing anything to cover your face would be effective at preventing transmission, many have now quietly dismissed that messaging.
Fauci specifically said that “cloth coverings work,” not just surgical or N95s. Former Surgeon General Jerome Adams famously suggested that rolling up a t-shirt in front of your face would be effective protection.
Yet public health departments and the media are now highlighting the importance of “high quality,” “well-fitted” masks.
Their desperation to justify masking has led to remarkably poor studies being released to support their anti-science messaging.
There is new research that has been released showing that masks are ineffective, regardless of type.
And it’s not just new research, it’s high quality research.
Finally, Another RCT on Mask Wearing
The Annals of Internal Medicine just published a randomized controlled trial comparing the ability of medical masks to prevent COVID infection to fit-tested N95s.
Importantly, this trial was conducted on healthcare workers who would be most likely to use masks appropriately.
To determine whether medical masks are noninferior to N95 respirators to prevent COVID-19 in health care workers providing routine care.
That trial design was also important as it was meant to determine whether or not N95 respirators were superior to “regular” surgical masks.
They examined 29 different health care facilities on multiple continents, from North America to Asia and Africa.
The percentage of healthcare workers testing positive for COVID in each group was tracked to determine how effective or ineffective higher-quality masking was in preventing infection.
Unsurprisingly, the results confirmed that there is essentially zero difference between surgical or N95 respirators when it comes to tests results.
In the intention-to-treat analysis, RT-PCR–confirmed COVID-19 occurred in 52 of 497 (10.46%) participants in the medical mask group versus 47 of 507 (9.27%) in the N95 respirator group (hazard ratio [HR], 1.14 [95% CI, 0.77 to 1.69]). An unplanned subgroup analysis by country found that in the medical mask group versus the N95 respirator group RT-PCR–confirmed COVID-19 occurred in 8 of 131 (6.11%) versus 3 of 135 (2.22%) in Canada (HR, 2.83 [CI, 0.75 to 10.72]), 6 of 17 (35.29%) versus 4 of 17 (23.53%) in Israel (HR, 1.54 [CI, 0.43 to 5.49]), 3 of 92 (3.26%) versus 2 of 94 (2.13%) in Pakistan (HR, 1.50 [CI, 0.25 to 8.98]), and 35 of 257 (13.62%) versus 38 of 261 (14.56%) in Egypt (HR, 0.95 [CI, 0.60 to 1.50]). There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group.
52 of 497 participants who wore medical masks got COVID-19, and 47 of 507 in the N95 group got COVID-19.
No matter how “high quality” your mask is, it’s entirely irrelevant.
The researchers also took pains to ensure that the control and treatment groups shared as many similarities as possible.
They excluded workers who could not pass a fit test, had laboratory-confirmed COVID, or “had received 1 or more doses of a COVID-19 vaccine with greater than 50% efficacy for the circulating strain.”
Yet none of that mattered; there was no difference in outcomes between the medical and N95 level masks.
The N95s in use were even specifically fit tested and approved respirators, far from the KN95s commonly used by the general public.
“Health care workers randomly assigned to the N95 respirator group were instructed to use a fit-tested National Institute for Occupational Safety and Health–approved N95 respirator when providing routine care to patients with COVID-19 or suspected COVID-19.”
It didn’t matter.
Even more importantly, these disappointing results were from facilities with universal masking policies in place.
Everyone, in each health care facility, “for all activities,” was required to wear masks.
The intervention included universal masking, which was the policy implemented at each site. This refers to the use of a mask when in the health care facility for all activities, whether patient related or not, including in workrooms, meetings, and treating persons that were not suspected or known to be positive for COVID-19.
It still didn’t work.
They even tracked potential exposure points, whether at home, in the community or in hospital exposures.
There was no difference.
What’s even more impressive about the futility of masking is that outside of Egypt, the observed results occurred before the more contagious Omicron variant emerged.
There were substantial differences in results between countries, which indicates the impact of N95s might have been further muted had it covered the Omicron period.
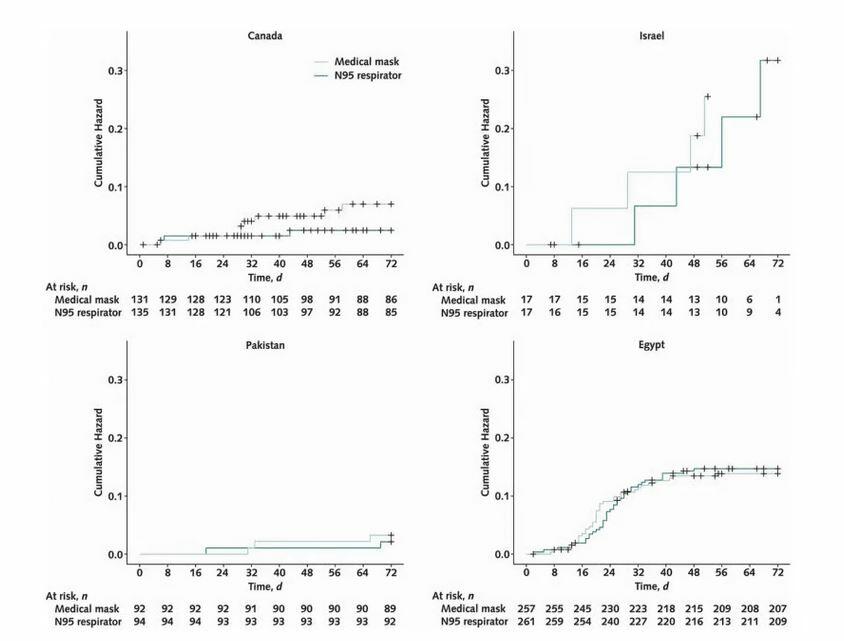
Canada, which was observed pre-Omicron, showed the biggest “benefit” to N95s, while post-Omicron Egypt was nearly identical.
It’s possible that the mild difference in Canada could have been erased entirely if subjected to the Omicron era.
On top of being functionally useless, N95s were substantially more likely to result in adverse effects.
According to the results page, there were significantly more reported issues in the respirator group:
“There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group.”
This becomes even more noteworthy since compliance with respirator masking was lower.
“Adherence with the assigned medical mask or N95 respirator was self-reported as “always” in 91.2% in the medical mask group versus 80.7% in the N95 respirator group and as “always” or “sometimes” in 97.7% in the medical mask group versus 94.4% in the N95 respirator group.”
While still extremely high, health care workers “always” wore N95s 80.7% of the time instead of 91.2% for medical masks.
This is one of the many issues the “experts” now pushing for (now disproven) “higher-quality” masking should address.
Health care professionals who are trained to use N95s can’t always use them yet experience higher rates of adverse effects.
Imagine how much worse compliance would be among the general public, especially if 13% are suffering significant side effects.
Results Show Expert Incompetence
This is yet another randomized controlled trial to show that masks do not work.
It also confirms the DANMASK study conducted earlier in the pandemic, which proved there was no benefit from masking in COVID prevention.
Even the Bangladeshi study, comparing villages, showed there was no benefit to masking at a population level. They used statistical misdirection and purposeful p-hacking to try and generate a positive result, and still could only get to a ~10% reduction for those over 50.
No matter the quality, no matter the compliance, masks are entirely ineffective at preventing transmission or infection.
The participants in this examination lived and worked in environments where universal masking was a requirement.
It didn’t matter.
This also examined health care workers, who, in theory, would be using and disposing of medical or N95 level masks properly.
There was no difference.
Now imagine how much worse the results would look for mask fanatics if it examined the Fauci-approved cloth coverings.
If “The Experts™” actually cared about following “the science,” or “the evidence,” this would once again be the nail in the coffin for masking.
More like the 40th nail in the coffin.
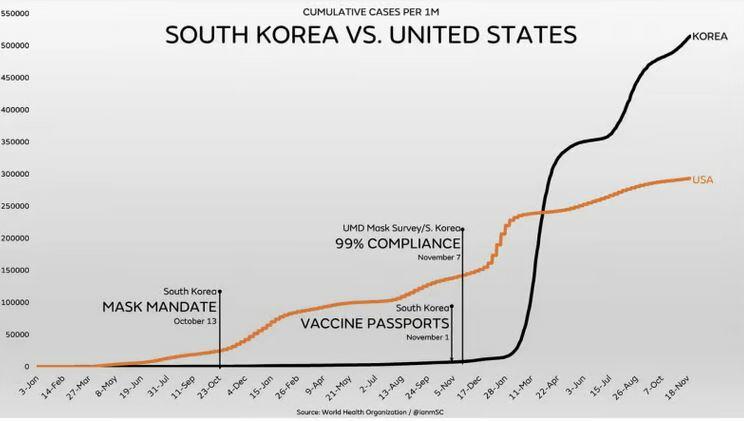
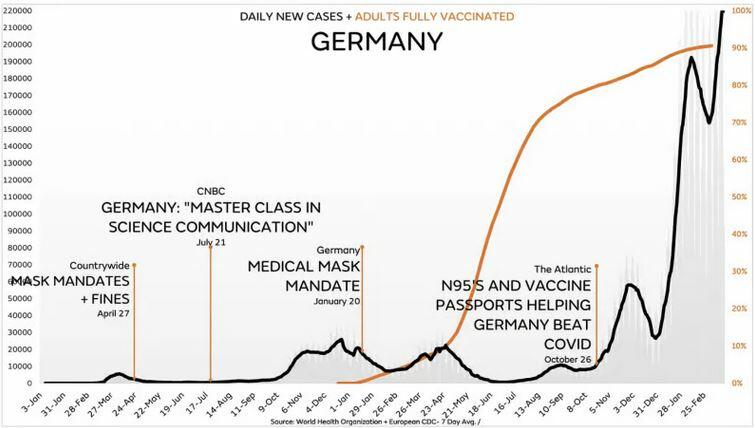
We have observational evidence through population-level comparisons that masks do not prevent the spread of COVID.
We also now have multiple randomized controlled trials confirming that masks do not prevent the spread of COVID.
And we have extremely well done comparisons of neighboring jurisdictions confirming it.
All the mask fanatics have is politically motivated wishful thinking, desperate advocacy from disproven CDC “studies,” and a commitment to avoiding reality.
Fauci and his health authority allies have lied to the public repeatedly about masking. The obsession with credentialism and appeals to authority within the media has resulted in tremendous, unjustified harm.
You’d hope that results like these would finally end their ridiculous posturing, but it’s abundantly clear they’re too dug in to ever relent.
But thankfully those paying attention now have even more ammunition in the fight for the inarguable scientific reality that masks do not work.
Authored by Ian Miller via the Brownstone Institute,

“The Experts™” have repeatedly tried to deflect from the failure of their policies with misdirection.
The reason lockdowns didn’t work in the United States or the United Kingdom is because they weren’t strict enough, according to many in the expert community.
Of course, their excuses have been conveniently ignored as China’s repressive zero COVID lockdowns have continued, with horrific consequences.
Now that mass protests have broken out in the country that “The Experts™” revered for their COVID handling, there’s a massive effort to disregard their own previous advocacy.
This is perhaps best exemplified by Canadian Prime Minister Justin Trudeau, who clearly used authoritarian measures to suppress the protests in his own country, while now supporting Chinese demonstrations.
— Defiant L’s (@DefiantLs) November 30, 2022
The bewildering lack of awareness of their own hypocrisy seems to be a feature of COVID-obsessed politicians and public health authorities.
Another similar, oft-repeated assertion is that the failure of universal masking can be explained by the type of masks being used by the public.
Even though the CDC and Dr. Fauci explicitly claimed that wearing anything to cover your face would be effective at preventing transmission, many have now quietly dismissed that messaging.
Fauci specifically said that “cloth coverings work,” not just surgical or N95s. Former Surgeon General Jerome Adams famously suggested that rolling up a t-shirt in front of your face would be effective protection.
Yet public health departments and the media are now highlighting the importance of “high quality,” “well-fitted” masks.
Their desperation to justify masking has led to remarkably poor studies being released to support their anti-science messaging.
There is new research that has been released showing that masks are ineffective, regardless of type.
And it’s not just new research, it’s high quality research.
Finally, Another RCT on Mask Wearing
The Annals of Internal Medicine just published a randomized controlled trial comparing the ability of medical masks to prevent COVID infection to fit-tested N95s.
Importantly, this trial was conducted on healthcare workers who would be most likely to use masks appropriately.
To determine whether medical masks are noninferior to N95 respirators to prevent COVID-19 in health care workers providing routine care.
That trial design was also important as it was meant to determine whether or not N95 respirators were superior to “regular” surgical masks.
They examined 29 different health care facilities on multiple continents, from North America to Asia and Africa.
The percentage of healthcare workers testing positive for COVID in each group was tracked to determine how effective or ineffective higher-quality masking was in preventing infection.
Unsurprisingly, the results confirmed that there is essentially zero difference between surgical or N95 respirators when it comes to tests results.
In the intention-to-treat analysis, RT-PCR–confirmed COVID-19 occurred in 52 of 497 (10.46%) participants in the medical mask group versus 47 of 507 (9.27%) in the N95 respirator group (hazard ratio [HR], 1.14 [95% CI, 0.77 to 1.69]). An unplanned subgroup analysis by country found that in the medical mask group versus the N95 respirator group RT-PCR–confirmed COVID-19 occurred in 8 of 131 (6.11%) versus 3 of 135 (2.22%) in Canada (HR, 2.83 [CI, 0.75 to 10.72]), 6 of 17 (35.29%) versus 4 of 17 (23.53%) in Israel (HR, 1.54 [CI, 0.43 to 5.49]), 3 of 92 (3.26%) versus 2 of 94 (2.13%) in Pakistan (HR, 1.50 [CI, 0.25 to 8.98]), and 35 of 257 (13.62%) versus 38 of 261 (14.56%) in Egypt (HR, 0.95 [CI, 0.60 to 1.50]). There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group.
52 of 497 participants who wore medical masks got COVID-19, and 47 of 507 in the N95 group got COVID-19.
No matter how “high quality” your mask is, it’s entirely irrelevant.
The researchers also took pains to ensure that the control and treatment groups shared as many similarities as possible.
They excluded workers who could not pass a fit test, had laboratory-confirmed COVID, or “had received 1 or more doses of a COVID-19 vaccine with greater than 50% efficacy for the circulating strain.”
Yet none of that mattered; there was no difference in outcomes between the medical and N95 level masks.
The N95s in use were even specifically fit tested and approved respirators, far from the KN95s commonly used by the general public.
“Health care workers randomly assigned to the N95 respirator group were instructed to use a fit-tested National Institute for Occupational Safety and Health–approved N95 respirator when providing routine care to patients with COVID-19 or suspected COVID-19.”
It didn’t matter.
Even more importantly, these disappointing results were from facilities with universal masking policies in place.
Everyone, in each health care facility, “for all activities,” was required to wear masks.
The intervention included universal masking, which was the policy implemented at each site. This refers to the use of a mask when in the health care facility for all activities, whether patient related or not, including in workrooms, meetings, and treating persons that were not suspected or known to be positive for COVID-19.
It still didn’t work.
They even tracked potential exposure points, whether at home, in the community or in hospital exposures.
There was no difference.
What’s even more impressive about the futility of masking is that outside of Egypt, the observed results occurred before the more contagious Omicron variant emerged.
There were substantial differences in results between countries, which indicates the impact of N95s might have been further muted had it covered the Omicron period.
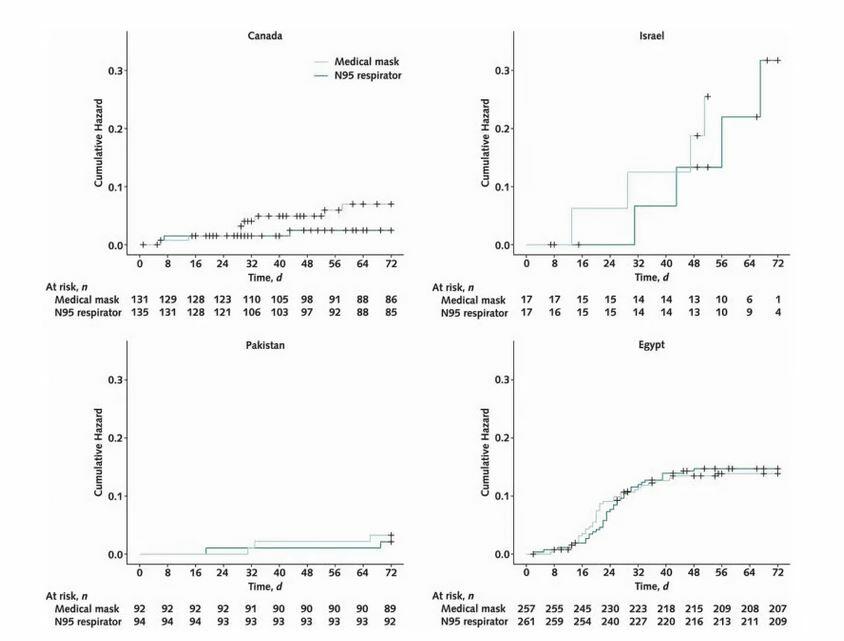
Canada, which was observed pre-Omicron, showed the biggest “benefit” to N95s, while post-Omicron Egypt was nearly identical.
It’s possible that the mild difference in Canada could have been erased entirely if subjected to the Omicron era.
On top of being functionally useless, N95s were substantially more likely to result in adverse effects.
According to the results page, there were significantly more reported issues in the respirator group:
“There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group.”
This becomes even more noteworthy since compliance with respirator masking was lower.
“Adherence with the assigned medical mask or N95 respirator was self-reported as “always” in 91.2% in the medical mask group versus 80.7% in the N95 respirator group and as “always” or “sometimes” in 97.7% in the medical mask group versus 94.4% in the N95 respirator group.”
While still extremely high, health care workers “always” wore N95s 80.7% of the time instead of 91.2% for medical masks.
This is one of the many issues the “experts” now pushing for (now disproven) “higher-quality” masking should address.
Health care professionals who are trained to use N95s can’t always use them yet experience higher rates of adverse effects.
Imagine how much worse compliance would be among the general public, especially if 13% are suffering significant side effects.
Results Show Expert Incompetence
This is yet another randomized controlled trial to show that masks do not work.
It also confirms the DANMASK study conducted earlier in the pandemic, which proved there was no benefit from masking in COVID prevention.
Even the Bangladeshi study, comparing villages, showed there was no benefit to masking at a population level. They used statistical misdirection and purposeful p-hacking to try and generate a positive result, and still could only get to a ~10% reduction for those over 50.
No matter the quality, no matter the compliance, masks are entirely ineffective at preventing transmission or infection.
The participants in this examination lived and worked in environments where universal masking was a requirement.
It didn’t matter.
This also examined health care workers, who, in theory, would be using and disposing of medical or N95 level masks properly.
There was no difference.
Now imagine how much worse the results would look for mask fanatics if it examined the Fauci-approved cloth coverings.
If “The Experts™” actually cared about following “the science,” or “the evidence,” this would once again be the nail in the coffin for masking.
More like the 40th nail in the coffin.
We have observational evidence through population-level comparisons that masks do not prevent the spread of COVID.
We also now have multiple randomized controlled trials confirming that masks do not prevent the spread of COVID.
And we have extremely well done comparisons of neighboring jurisdictions confirming it.
All the mask fanatics have is politically motivated wishful thinking, desperate advocacy from disproven CDC “studies,” and a commitment to avoiding reality.
Fauci and his health authority allies have lied to the public repeatedly about masking. The obsession with credentialism and appeals to authority within the media has resulted in tremendous, unjustified harm.
You’d hope that results like these would finally end their ridiculous posturing, but it’s abundantly clear they’re too dug in to ever relent.
But thankfully those paying attention now have even more ammunition in the fight for the inarguable scientific reality that masks do not work.





